The mitral valve (MV) is a valve in the heart between the left atrium and left ventricle. Its function is to close when the heart is contracting (systole) and open when the heart is relaxed(diastole).
The mitral valve is a complex valve made up of the annulus, leaflets (anterior and posterior), papillary muscles and chords. All components of this valve must function properly for the valve to be competent.
Diseases that can affect the mitral valve can be broadly divided into narrowing of the valve called mitral stenosis (MS) or leak called mitral regurgitation (MR).
Mitral stenosis is mostly caused by a condition called rheumatic heart disease. The disease makes the valve leaflets stiff and unable to open properly. This results in back pressure in the left atrium. In most severe situation MS can result in lung congestion and heart failure. Mitral valve stenosis may be repaired when discovered early. If the condition is too advanced, then mitral valve replacement would be procedure of choice.
Mitral regurgitation can be caused by degenerative, ischemic or infective heart disease. Any part of the mitral valve complex component that is damaged will result in the mitral valve leaking. The degree of leak may be graded with echocardiography (ultrasound investigation of the heart).
If the leak is moderately severe, your cardiologist may refer you for surgical repair. Surgical repair can be done with multiple well described techniques and the findings on echocardiography will determine whether the valve is reparable. Artificial chords to replace torn chords, annuloplasty rings to reduce the size of the mitral valve are some of the more common methods for MV repair. If repair is not possible, then similar to MS, MV replacement has to be performed. Depending on suitability, minimally invasive mitral valve repair can be performed.
Mr. A
51 male
Well previously, active sportsman. Plays badminton and golf.
Sudden onset of shortness of breath and palpitations (feeling of fast heart beat in the chest)
Admitted to hospital. Seen by a cardiologist.
ECG showed atrial fibrillation (Fig. 1), highly irregular heart beat at fast heart rate.
Chest x ray : heart size enlarged, fluid seen in the lung bases
Echocardiography: severe mitral valve regurgitation (leak), flail posterior leaflet. Left atrium size enlarged, left ventricle size also enlarged.
Dilated left ventricular cavity size with normal left ventricular systolic function. LVEF 65-70%
No regional wall motion abnormality. No left ventricular hypertrophy. Bilateral dilatation. No obvious Intracardiac clot seen.
Posterior mitral valve prolapse with flail P2,P3 segments and severe mitral regurgltation (eccentric jet) Aortic valve thickening with trivial aortic regurgltation.
Rest of cardiac valves appear normal. Mild tricuspid regurgitation.
Intact Interatrial and interventricular septum with no obvious Intracardiac shunt.
Great vessels normal. Pericardium normal. Normal pulmonary artery pressure. PASP 33mmHg (Assuming RAP 5mmHg)
Posterior mitral valve prolapse with flail P2,P3 segments and severe mitral regurgltation (eccentric Jet) Dilated left ventricular cavity size with normal left ventricular systolic function. LVEF 65-70% Aortic valve thickening with trivial aortic regurgitation.
Mitral valve regurgitation (Fig. 2) is a condition where the valve between the left atrium (upper chamber) and left ventricle (the main pumping chamber of the heart) is leaking. This results in backflow of blood to the left atrium whenever the left ventricle beats. There are four grades of regurgitation, none, mild, moderate, severe.
When the grade is severe, there will be excess pressure and volume of blood into the left atrium. This can result in heart failure, causing shortness of breath as seen in this patient. The chest x ray findings are consistent with back pressure in the lungs and fluid in the lung bases.
Over time, the left atrium enlarges. The left ventricle also enlarges, when there is too much volume per heart cycle.
The palpitations can be explained with the ECG findings of atrial fibrillation. This condition occurs when mitral regurgitation is severe and cause the left atrium to be stretched. The abnormal rhythm is atrial fibrillation which makes the heart beat fast up to 120-130 beats per minute. This needs to be treated medically or in certain cases by a surgical technique called maze procedure.
The patient Mr. A was referred to myself for discussion on surgical treatment.
I recommended mitral valve repair, with maze procedure.
Surgical intervention is indicated for the following reasons:
1. Mitral Regurgitation is graded as severe
2. The left ventricle and left atrium is noted to be dilated which implies volume loading of the heart chambers.
3. There are symptoms of heart failure (shortness of breath)
4. Presence of atrial fibrillation which indicates the heart is grossly affected by the mitral valve disease.
The risk of this procedure is 2% mortality, 1% risk of stroke. Success rate post mitral valve repair is 98%. Success rate for post maze procedure is 90%.
Prior to any valve surgery, a patient above the age of 40 years for males and 45 years for females, will need to undergo a coronary angiogram, which is a minor procedure involving a catheter inserted into the coronary arteries of the heart. This will allow us to detect the presence of any coronary artery disease.
For Mr A, this was normal. No significant coronary artery disease was detected.
He underwent open heart surgery. The mitral valve was repaired with resection of P2 part of the posterior leaflet(Fig. 3) and a band. Together with valve repair, he also had a maze procedure. This corrects the atrial fibrillation and restores the normal sinus rhythm.
He recovered very well from heart surgery. Hospital stay was 1 week.
Now at three months after surgery, he is able to resume playing golf and badminton.
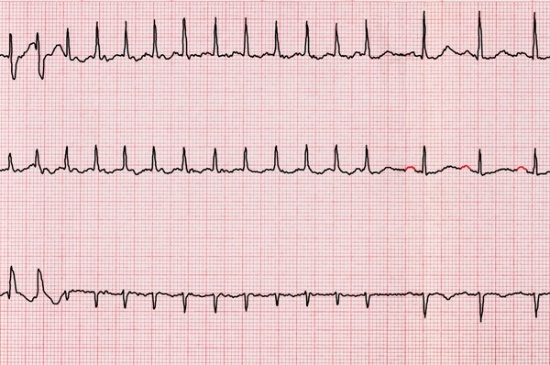
Fig.1 ECG showing abnormal rhythm of atrial fibrillation with fast heart rate resulting in palpitations.
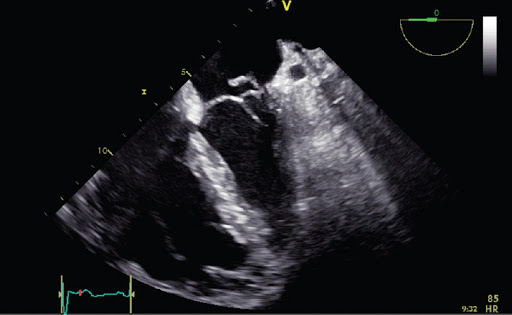
Fig.2 Typical echocardiography showing mitral valve leak and flail leaflet
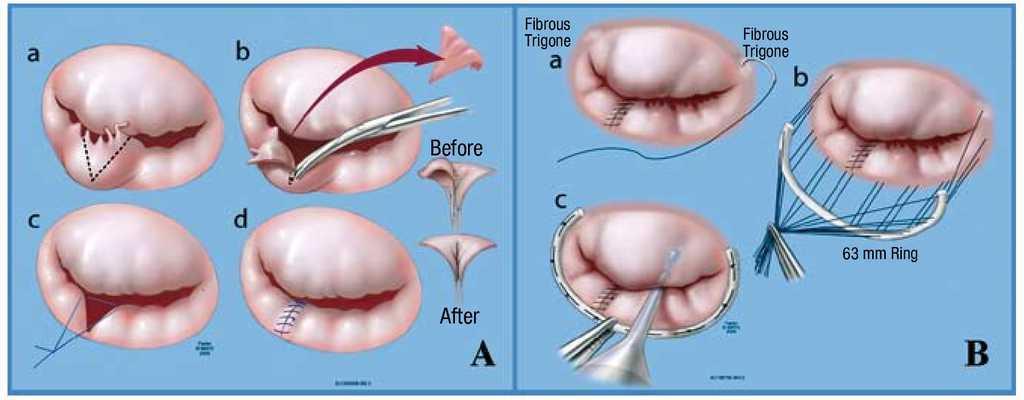
Fig.3 Mitral valve repair with leaflet resection and band